Participant Info
- First Name
- Zeeshan
- Last Name
- Mahfooz
- Designation
- Radiologist
- Department
- Radiology
- Instituition
- Family health hospital Islamabad
- dr_zeeshan@hotmail.co.uk
- Cell Phone #
- 3332327203
- PMDC #
- 38183-S
- Address
- House no 389 street no 38A sector I/9-4
- City
- Islamabad
- Accommodation Required?
- No
- Accomodation Type
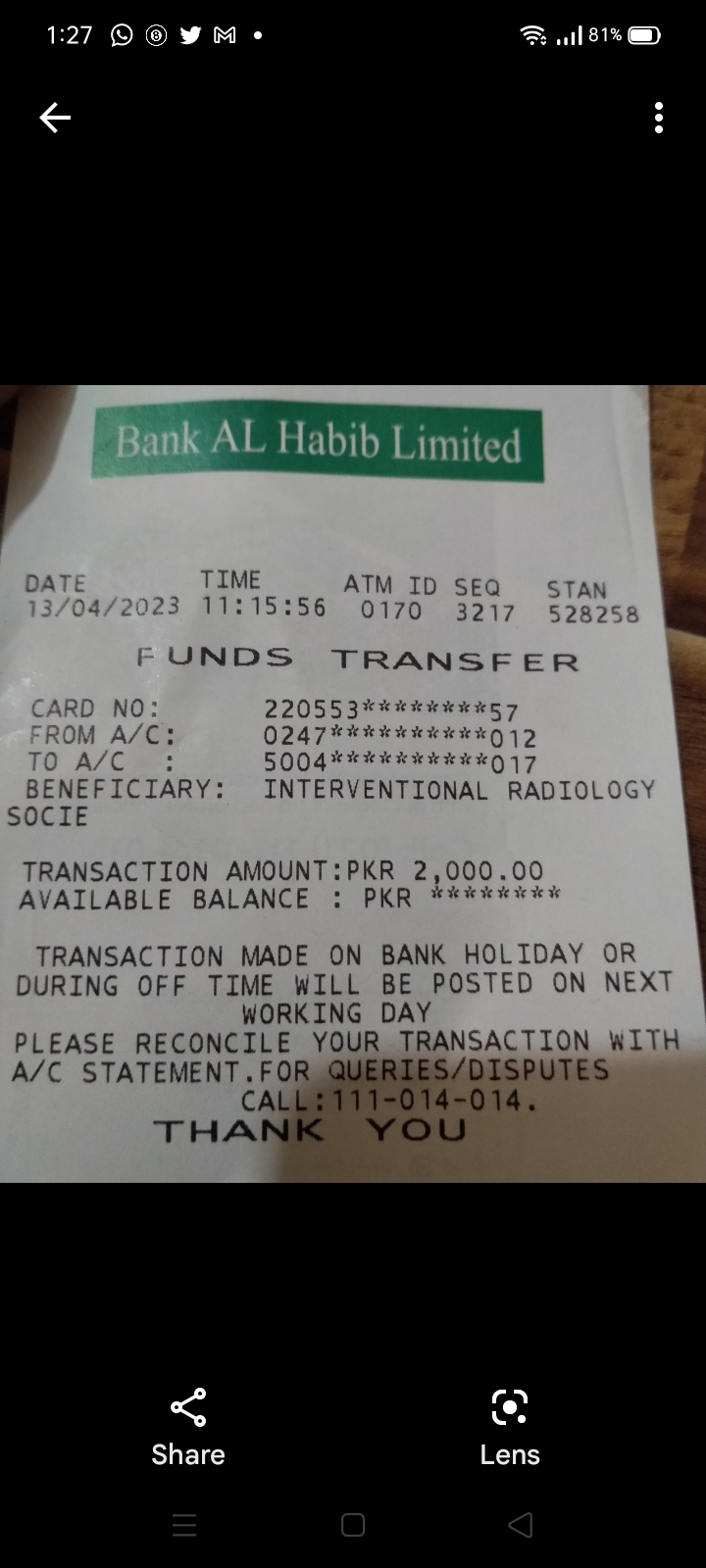
- Payment Status
- I have already paid
- Sponsoring Institution/Company Name
- Fee Deposit Proof